|
Psychology and Psychotechnics
Reference:
Griber, Y.A., Delov, A.A., Kovalev, P.S. (2024). Color vision of people with headaches. Psychology and Psychotechnics, 2, 66–82. https://doi.org/10.7256/2454-0722.2024.2.70470
Color vision of people with headaches
Griber Yuliya Alexandrovna
Doctor of Cultural Studies
Professor, Director of Color Laboratory at Smolensk State University
214000, Russia, Smolensk region, Smolensk, Przhevalskogo str., 4

|
y.griber@gmail.com
|
|
 |
Other publications by this author
|
|
Delov Aleksey Alekseevich
ORCID: 0000-0001-8589-8523
Researcher at the Color Laboratory of Smolensk State University
214000, Russia, Smolensk region, Smolensk, Przhevalsky str., 4
|
|
aleksejdelov@gmail.com
|
|
 |
|
Kovalev Pavel Sergeevich
ORCID: 0000-0002-1223-8812
Researcher at the Color Laboratory of Smolensk State University
214000, Russia, Smolensk region, Smolensk, Przhevalsky str., 4
|
|
rozdavid2009@yandex.ru
|
|
 |
|
DOI: 10.7256/2454-0722.2024.2.70470
EDN: HIHAPG
Received:
16-04-2024
Published:
26-06-2024
Abstract:
The aim of the study is to obtain new data on possible changes in color vision of people with headaches. The object of the study is people who periodically experience primary headaches of different nature. The subject of the study is the specificity of perception of chromatic parameters of the environment and color sensitivity of people with headaches of different nature, quality, intensity and frequency. The data were collected using the Farnsworth-Munsell standard clinical color vision test (FM-100). The study involved 65 people aged 17 to 66 years. The results of the assessment of color vision in the experimental group were compared with the normative indicators and data obtained in the age-matched control group (N=40). Special attention was paid to discussing the possible causes of the identified disorders and analyzing the correlation between various aspects of headache with individual indicators of color sensitivity. The data analysis included calculating the total error (TES), as well as partial errors (PES) along the blue-yellow (B-Y) and red-green (R-G) axes. We also identified partial errors for individual tones. The study revealed a noticeable specificity in the perception of blue-green and blue shades of patients with severe, chronic and non-localized headaches. Since the detected color vision disorders appear to be temporary and are most likely typical of the premonitory phase of headaches, the results of this study may contribute to understanding of headache predictors. Since the identified changes relate to only one group of (blue) shades, the findings of the study can be used in the development of alternative treatment methods. In particular, in choosing the optimal color of tinted lenses, which are offered to patients to relieve headaches and reduce their frequency.
Keywords:
color vision, headaches, FM-100 test, color sensitivity, color discrimination, color, color cognition, color perception, visual trigger, visual perception
This article is automatically translated.
Introduction Headaches in the modern world are among the most common diseases of the nervous system. According to epidemiological studies, 62% of Russian residents suffer from recurrent headaches [1] and about 50-75% of the adult population of the entire Earth [2]. Despite some regional differences, headaches are a global problem affecting people of all races, income levels and geographical regions [3]. People experiencing headaches constantly report similar visual triggers that can cause them to have a new attack. Certain visual qualities of the environment have a noticeable effect on their well-being (see appendix: [4]). Among the most significant are certain characteristics of natural and artificial lighting [5; 6], flickering light [7], certain visual images [8], the specific structure of the interior space of premises and workplaces [4]. Awareness and avoidance of these and other provoking factors is important not only in comprehensive headache treatment programs as part of a therapeutic regimen, but also in designing a "liveable" environment (see research review: [9-11]). Therefore, over the past few decades, clinical specialists and scientific researchers have been studying with special interest the relationship of various aspects of headache with individual components of the visual system. Special attention is paid to the parameters of visual discomfort, which is sometimes called "visual stress" or simply "sensitivity" (to patterns, glare, colors, etc.) (see e.g.: [12]). The interest in this issue is largely explained by the fact that there seems to be a connection between the visual triggers of headache and the feeling of visual discomfort. As a rule, people who are susceptible to visual headache triggers also experience greater discomfort when viewing trigger stimuli [13; 14]. The data already obtained also indicate that there is a connection between visual discomfort and color sensitivity – the ability to perceive different shades of color with different spectral composition of radiation (see e.g. [15]). At the same time, the theory of efficient coding is gaining increasing empirical support [12], according to which visual stress is caused by shades that differ significantly from the usual ones – those that are usually found in the natural environment surrounding a person (see appendix: [16]). Studies show that in people suffering from headaches, color sensitivity does not coincide with the age-appropriate control group. The differences relate to the perception of pink [8], red [17], blue and purple shades [18]. Some groups of bright shades (primarily saturated and intense red and orange) are strong visual triggers for patients with chronic headaches that can provoke a new attack [7]. The effect of tinted lenses on the feeling of visual discomfort and the frequency of headaches has also been established. In particular, subjects who constantly wore glasses with colored lenses were less likely to have headaches compared to participants from the control group [5; 19]. A similar corrective effect on the feeling of visual discomfort was also provided by a colored background for a computer screen [13)]. At the same time, a review of the works published so far proves that the analysis of color sensitivity in people with headaches, in the vast majority of cases, is limited to patients with migraines (see, for example.: [7; 8; 13; 14; 17; 18]). As far as we know, comprehensive studies of color perception in people with other types of headaches have not yet been conducted. Only a few isolated cases of specific color sensitivity in people with cluster headaches have been described [5; 19]. In this article, we will continue to study the specifics of perception of chromatic environmental parameters and color sensitivity. The purpose of the article is to obtain new data on possible changes in color vision in people with primary headaches. According to statistics, primary headaches account for 95-97% of all cases [20]. Unlike secondary (symptomatic) headaches, they are characterized by the absence of organic damage to the brain, head and neck structures. The most well-known form of primary headaches is migraine. However, at the same time, it is by no means the most common and in Russia accounts for only 14% of all cases. Along with migraine, primary headaches include many other forms, including tension headache, trigeminal autonomic cephalgia, cough pain, headache associated with physical exertion, sexual exertion [21]. The hypothesis of the study is that in people experiencing recurrent primary headaches of different nature, the perception of chromatic environmental parameters and color sensitivity changes; differences may correlate with the experience of headaches, the frequency of their occurrence, the nature and quality of the pain experienced, their intensity and localization. Research materials and methods (1) Participants The study involved 65 people (13 men and 52 women) aged 17 to 66 years (average age 26.3, SD=12.1). All of them have recently experienced headaches of varying intensity, nature and quality, which they experienced with varying frequency. On average, the experience of headaches was 10.64 years (minimum – 1 year, maximum – 46 years, SD=10.10). The results of the assessment of color vision in the experimental group were compared with the normative indicators [22-24] and the data obtained in the age-matched control group (N=40, average age 23.54, SD=8.4, 12 men and 28 women). All study participants had normal or normalized visual acuity.
Before starting the study, each of the participants independently filled out a detailed questionnaire that included an expanded set of questions about various aspects of headaches. The questions concerned the temporal pattern of headaches (time from the moment of the first and last attack, duration and frequency of attacks), the nature, quality and intensity of pain, established triggers, and the presence of accompanying symptoms. (2) Color vision assessment procedure Data collection was carried out using the standard clinical Farnsworth-Munsell color vision test for 100 shades (Farnsworth-Munsell 100-hue test, FM-100) [25; 26]. In the practice of scientific and clinical research, this test is traditionally used to diagnose the type and severity of acquired color vision disorders caused by various pathologies of the visual system (including maculopathy, glaucoma, optic neuritis, cataracts), systemic diseases (such as diabetic retinopathy or hypothyroidism), as well as the influence of various kinds of extreme changes in the environment the environment affects human visual perception (for example, by an extreme decrease in natural light beyond the Arctic circle) (see research review: [27]). The FM-100 test contains 85 shades, which together form a complete color circle. The shades are separated by approximately equal perceptual steps. They differ only in tone and have the same lightness and saturation (Value 6 and Chroma 6 in the symbols of the Mansell system). The chips are stored in four pencil cases, which are often designated with the Latin letters A, B, C and D. There are 22 chips in pencil case A, and 21 in the other three. In each of the four pencil cases, the chips represent a certain sector of the color circle: from red to red-orange (pencil case A, chips 85-21), from yellow to yellow-green (pencil case B, chips 22-42), from green to green-blue (pencil case C, chips 43-63) and from indigo to magenta (pencil case D, chips 64-84). The extreme chips in each of the pencil cases are fixed, the rest are movable. Each participant in the study was asked to arrange the chips in the pencil cases in such a way that the transition from one shade fixed at the end of the pencil case to the other was as smooth as possible. In accordance with the recommendations for people with neurological disorders (see, for example: [18]), the time for completing the task was not limited. (3) Data analysis The data was analyzed using specialized computer programs. The analysis included calculating the total error (TES) and calculating partial errors (PES) along the blue-yellow (B-Y) and red-green (R-G) axes. Partial errors for individual tones were also calculated. (3.1) Total Error (TES) is an indicator that is used to assess the quality of color differentiation in general. It is calculated as the sum of the points for the chips in the four boxes. The score for an individual chip is calculated as the sum of the absolute difference between the error value for a given color and the error values of neighboring chips minus 2 [26]:  , where i is the number of the pencil case; Cj is the number of the chip j; CEj is the error of the chip j; n is the number of movable chips in the pencil case corresponding to i (n = 22 for pencil case A, and n = 21 for pens B–D). If all the chips are in the correct order, the value of the total error TES =0; the more offsets the chips, the higher the TES score. Since TES has an asymmetric distribution, calculations often use the square root of the total number of errors (√TES) to obtain a distribution closer to normal [24]. (3.2) Partial errors (PES) were calculated for individual shade ranges: (1) along the axes: blue-yellow B-Y axis (chips 1-12, 34-54 and 76-85); red-green R-G axis (chips 13-33 and 55-75); (2) for individual tones: from red to yellow-red R-YR (chips 1-9); from yellow-red to yellow YR-Y (chips 10-17); from yellow to yellow-green Y-GY (chips 18-26); from yellow-green to green GY-G (chips 27-35); from green to blue-green G-BG (chips 36-45); from blue-green to blue BG-B (chips 46-53); from blue to blue-purple B-PB (chips 54-60); from blue-purple to purple PB-P (chips 61-70);
from purple to purple-red P-RP (chips 71-77); from purple-red to red RP-R (chips 78-85). Results General Error (TES) In the majority of patients experiencing headaches (80%), color vision corresponded to their age norm (Table 1). In 11 participants (17%), the value of the total number of errors exceeded the average value for healthy normal trichromates, but it was still within the upper limit. Only two people (a woman, 19 years old, and a man, 25 years old, both experience frequent headaches) had slightly worse color vision than normal (√TES=10.58 and √TES=9.59, respectively). Table 1. The mean value and standard deviation of the square root of the total number of errors (√TES) for healthy normal trichromates, presented in [22, Table 1],[23, Table 1]) and [24, Table 1] 
We found a positive correlation between the frequency of headache occurrence (episodic, frequent, chronic) and the value of the total error score (√TES) (Fig. 1). On average, this indicator in people with episodic pain was 4.18 and turned out to be even lower than in the control group, where √TES=4.92. In people experiencing frequent and chronic pain, the magnitude of the total error (√TES) was noticeably higher and amounted to 5.51 and 5.83, respectively. 
Fig. 1. Correlation between the frequency of headache occurrence (episodic, frequent, chronic) and the value of the total error score (√TES) The correlation between the magnitude of the total error score (√TES) and the intensity of the headache was also even more significant. In patients with mild, moderate and severe headaches, this indicator was 3.89, 4.54 and 6.53, respectively (Fig. 2). 
Fig. 2. Correlation between headache intensity (mild, moderate, severe) and the value of the total error score (√TES) In addition, the value of the total error score (√TES) correlated with the localization of headaches. In patients with localized pain, this indicator was lower on average than in patients who experienced pain without a specific localization (√TES=4.65 and √TES=5.56, respectively). We did not find a statistically significant correlation between the experience of headaches and the value of the total error score (√TES) (Fig. 3). 
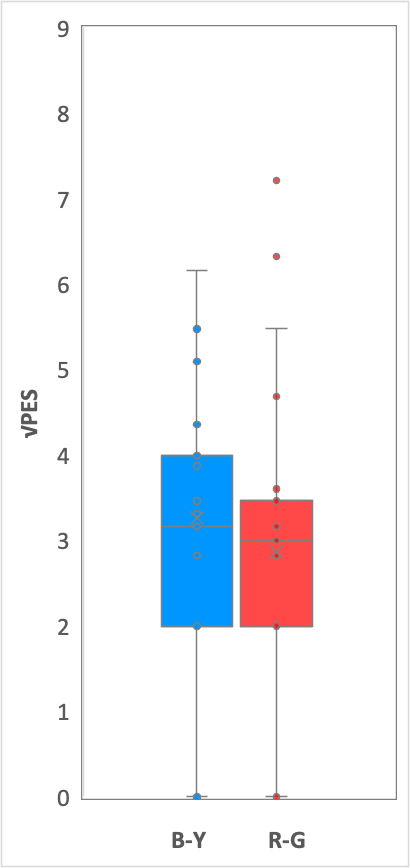
Fig. 3. The function of headache experience and the value of the total error score (√TES) The correlation of the total error score (√TES) with age, gender, nature and quality of headaches (aching, pressing, throbbing, acute, bursting), normal behavior during an attack (drowsiness, emotional arousal, anxiety, fear) and heredity of headaches also turned out to be statistically insignificant. Partial errors (PES) along the blue-yellow and red-green axes In patients with frequent (from two to ten attacks per month) and chronic (more than ten attacks per month) headaches, errors along the blue-yellow (B-Y) axis prevailed among partial errors (√PES) (Fig. 4). In patients with frequent pain, the average value of √PES (B-Y) was 4.07; the average value of √PES (R-G) was 3.53. In patients with chronic pain, the average value of √PES (B-Y) reached 4.43; the average value of √PES (R-G) was 3.50. | 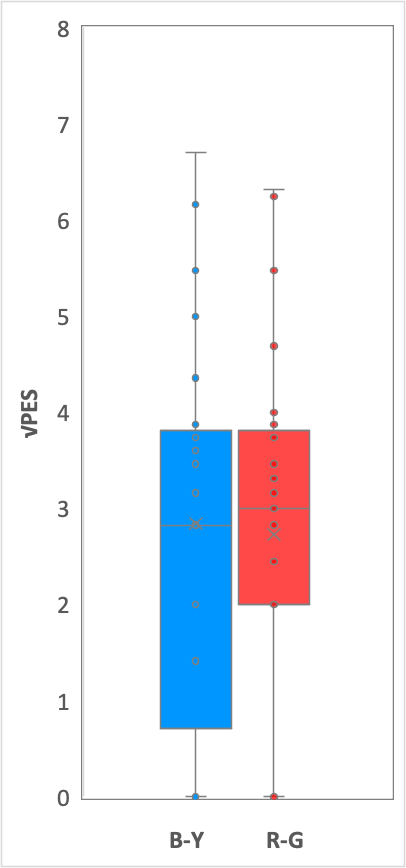
| 
| 
| | Episodic pain | Frequent pain |
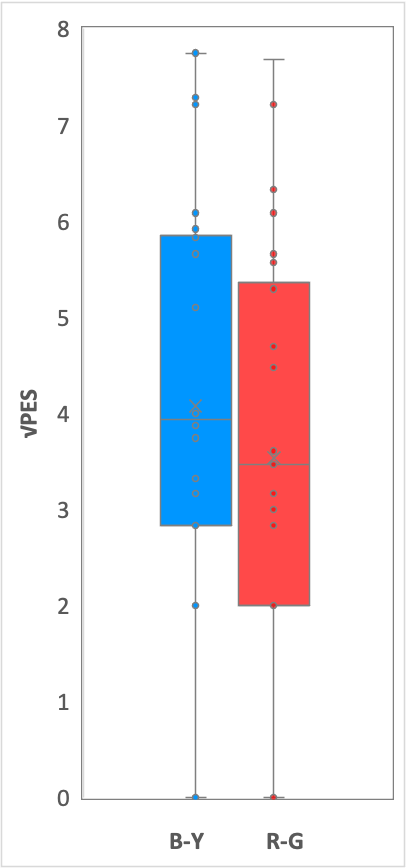
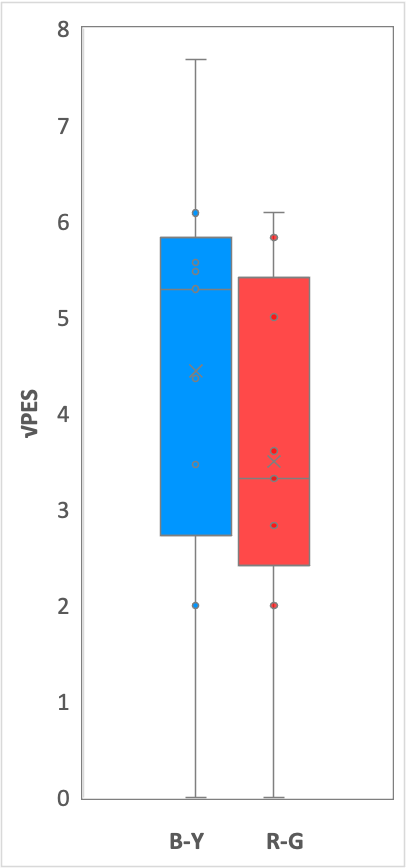
Chronic pain | Fig. 4. Partial errors (√PES) along the blue-yellow (B-Y) and red-green (R-G) axes in patients with different frequency of headaches A similar pattern was found in participants with moderate to severe pain (Fig. 5). In subjects with moderate pain, the average value of √PES (B-Y) was 3.27; the average value of √PES (R-G) was 2.86. In patients with severe pain, the average value of √PES (B-Y) It reached 4.96; the average value of √PES (R-G) was 4.07. | 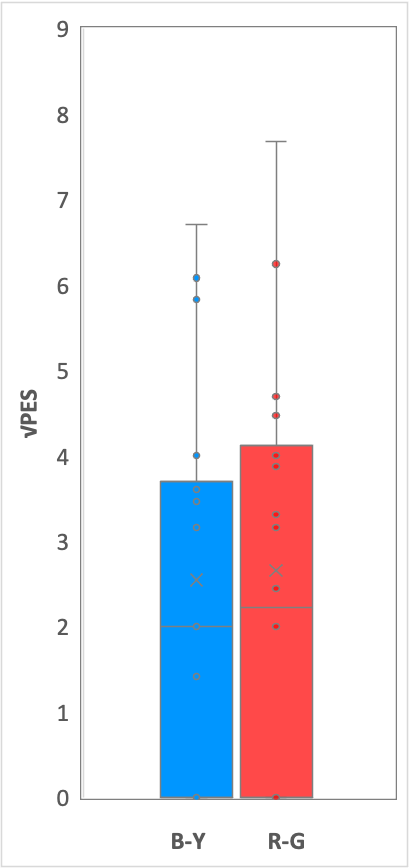
| 
| 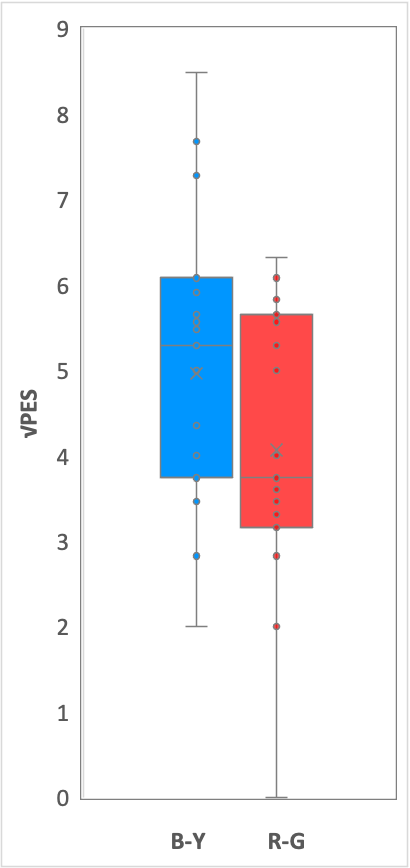
| | Mild pain | Moderate pain | Severe pain | Fig. 5. Partial errors (√PES) along the blue-yellow (B-Y) and red-green (R-G) axes in patients with different headache intensity A similar predominance of errors along the blue-yellow axis was also described in the study by A. Shepherd [18] for people with migraine. However, in this experiment, the difference with the red-green axis turned out to be statistically insignificant, and the relationship between the frequency of pain, their intensity and nature was not recorded. In the control group, such a difference between the number of errors along the blue-yellow and red-green axes was statistically insignificant: the average value of √PES (B-Y) was 3.49; the average value of √PES (R-G) was 3.21. Partial errors (PES) for individual tones The most noticeable increase in the number of errors, compared with the control group, was recorded in patients experiencing frequent and chronic pain for blue-green and blue shades (BG-B). 
Fig. 6. The average value of the partial error (Mean PES) for individual tones in patients with different frequency of headaches (green lines) and in the control group (red line) The number of errors for individual tones was also correlated with the intensity of headaches. In patients experiencing severe pain, there was a noticeable increase in the number of errors in the range from green to blue (G-BG and BG-B) (Fig. 7). 
Fig. 7. The average value of the partial error (Mean PES) for individual tones in patients with different headache intensity (blue lines) and in the control group (red line) Patients with non-localized headaches made more mistakes in the green, blue-green, blue and purple-red hue ranges compared with the control group and with study participants whose pain was localized (Fig. 8). 
Figure 8. Mean partial error (Mean PES) for individual tones in patients with varying degrees of headache localization (gray lines) and in the control group (red line) Discussion and conclusions The study showed a noticeable specificity in the perception of blue-green and blue shades in patients with severe, chronic and non-localized headaches.
The most significant changes in color perception were noted for blue shades in subjects with chronic pain. All of these people experience more than 10 seizures per month and experienced the last attack a few days before the start of the study. Based on this frequency, we can assume that the color discrimination disorder noted in them could not be a consequence of an attack suffered before the start of testing, but a predictor of a new one. A similar violation of the perception of blue in the premonitory phase was noted in other previously conducted experimental studies of migraine, according to which a reduced perception of blue was observed only in patients who experienced an attack within 72 hours immediately after testing [17]. To date, there is no clear answer to the question of the causes of color vision disorders in people suffering from headaches. Color differentiation is a complex process involving retinal, subcortical and cortical components. At the lowest level of visual signal processing, light is absorbed by three cone photoreceptors of the L-, M- and S-type, which respond to long (or red), medium (green) and short (blue) waves, respectively. In the retina, the signals are converted into two opposing channels L ± M (red-green) and S-(L + M) (blue-yellow). The antagonism of cones persists in the retinofugal visual pathways at least up to the primary visual cortex (V1). The presence of these two channels leads to the appearance of two physiologically important sets of colors in any color space. These colors form the so-called "cardinal" color directions, since in each case they stimulate one and only one cone-shaped pathway connecting the retina and cortex (see e.g.: [13]). To assess the sensitivity of the cone photoreceptors of the retina, the calculation of the number of errors along the blue-yellow and red-green axes is traditionally used. When perceiving shades along the blue-yellow axis, only the signal from the S-type cones changes, the signals from the L- and M-cones remain constant. Along the red-green axis, on the contrary, the signal from the S-cones remains unchanged, but the ratio of activity of the L- and M-cones changes. Accordingly, the partial error indicator along the blue-yellow axis (PES(B-Y)) allows you to evaluate the sensitivity of S-type cones, along the red-green (PES(R-G)) – the sensitivity of L- and M-cones. In our study, it was found that the differences in color perception between the group with headaches and the control group mainly relate to the blue-yellow axis, i.e. they are limited to shades selective for S-type cone photoreceptors. In previous studies, no differences were found for shades selective for L- and M-type cones (see sub-section: [18]). Patients with migraine examined between attacks had a similar deficiency in sensitivity to short wavelengths [28]. The revealed changes in color perception hardly reflect changes in the work of the retina or photoreceptors. Since the decrease is limited exclusively to one group of shades, it most likely occurs at the precortical stage or at the stages preceding the unification of signals from cone-opponent signals (cf.: [18]). Similar disturbances in the perception of blue color are characteristic of the early stages of diseases with retinal dysfunction, such as glaucoma and diabetes, while impaired perception of red color seems to be more common in diseases with damage to the foveal region (see appendix: [17]). On the other hand, there is some reason to assume that the detected disorders may be related to the work of the dopaminergic system. Studies show that this system is directly related to headaches and migraines [29]. In particular, a migraine attack may be preceded by precursor symptoms, which are believed to be associated with dopaminergic dysfunction. These symptoms, which may occur 3 days before the attack and earlier, include changes in mood, behavior, alertness, appetite and intestinal activity (see appendix: [17]). In light of these observations, the decrease in blue color perception that we observed in patients with chronic headaches shortly before an attack may be an expression of the precursor phase of the attack, which is characterized by dopaminergic dysfunction. This interpretation may be consistent with clinical evidence that impaired perception of blue color is also noted in Parkinson's disease [30; 31]. At the same time, it is suggested that in such patients, an acquired defect in the perception of blue color may originate at the retinal level, since in Parkinson's disease dopaminergic neurons can degenerate both in the retina and in the brain stem. Since the detected color vision disorders appear to be temporary and are most likely typical of the premonitory phase of seizures, the results of this study may contribute to further study of predictors of headache. The new data obtained on changes in color vision may be useful for understanding not only the pathophysiology of headache. Since the identified changes relate to only one group of (blue) shades, the findings of the study can be used in the development of alternative treatment methods. In particular, to choose the optimal color of tinted lenses, which are offered to patients to relieve headaches and reduce the frequency of seizures [5; 19].
References
1. Saylor, D., & Steiner T. J. (2018). The global burden of headache. Seminars in Neurology, 38(2), 182–190. Retrieved from https://doi.org/doi:10.1055/s-0038-1646946
2. Tabeeva, G. R. (2022). Headaches in general medical practice. Terapevticheskii Arkhiv, 94(1), 114–121. Retrieved from https://doi.org/10.26442/00403660.2022.01.201325
3. GBD 2021 Nervous System Disorders Collaborators. (2024). Global, regional, and national burden of disorders affecting the nervous system, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. The Lancet. Neurology, 23(4), 344–381. Retrieved from https://doi.org/10.1016/S1474-4422(24)00038-3
4. Friedman, D. I., & De ver Dye, T. (2009). Migraine and the environment. Headache, 49(6), 941–952. Retrieved from https://doi.org/10.1111/j.1526-4610.2009.01443.x
5. Wilkins, A., & Cooper, N. (2021). Treatment of cluster headache in a different light: a case study. touchREVIEWS in Neurology, 17, 110–111. Retrieved from https://doi.org/10.17925/USN.2021.17.2.110
6. Bernstein, C. A., Nir, R. R., Noseda, R., Fulton, A. B., Huntington, S., Lee, A. J., Bertisch, S. M., Hovaguimian, A., Buettner, C., Borsook, D., & Burstein, R. (2019). The migraine eye: distinct rod-driven retinal pathways' response to dim light challenges the visual cortex hyperexcitability theory. Pain, 160(3), 569–578. Retrieved from https://doi.org/10.1097/j.pain.0000000000001434
7. Hadjikhani, N., & Vincent, M. (2021). Visual perception in migraine: a narrative review. Vision, 5(2), 20. Retrieved from https://doi.org/10.3390/vision5020020
8. Hine, T. J., & White, Y. B. Z. (2022). Pattern-induced visual discomfort and anxiety in migraineurs: their relationship and the effect of colour. Vision, 6(1), 1. Retrieved from https://doi.org/10.3390/vision6010001
9. Griber, Y. A., Selivanov, V. V., Weber, R. (2020). Color in the educational environment for older people: recent research review. Perspektivy nauki i obrazovania – Perspectives of Science and Education, 47(5). Р. 368–383. Retrieved from https://doi.org/10.32744/pse.2020.5.26
10. Griber, Y. A. (2021). Cvet, udobnyj dlya zhizni [A livable colour]. Project Baikal, 18(67), 82–87. Retrieved from https://doi.org/10.51461/projectbaikal.67.1759
11. Griber, Y. A. (2022). Cvet iznutri: novyj vektor issledovaniya gorodskoj koloristiki [Color from within: а new vector in the studies of urban coloristics]. Project Baikal, 19(71), 144–149. Retrieved from https://doi.org/10.51461/projectbaikal.71.1956
12. Penacchio, O., Haigh S. M., Ross, X., Ferguson, R., & Wilkins, A. J. (2021). Visual discomfort and variations in chromaticity in art and nature. Frontiers in Neuroscience, 15, 711064. Retrieved from https://doi.org/10.3389/fnins.2021.711064
13. Shepherd, A. J., Hine, T. J., & Beaumont, H. M. (2013). Color and spatial frequency are related to visual pattern sensitivity in migraine. Headache, 53(7), 1087–1103. Retrieved from https://doi.org/10.1111/head.12062
14. Shepherd, A. J. (2020). Tracking the migraine cycle using visual tasks. Vision, 4(2), 23. Retrieved from https://doi.org/10.3390/vision4020023
15. Westland, S., & Maggio, M. (2023). Universal Principles of Color: 100 Key Concepts for Understanding, Analyzing, and Working with Color. Beverly: Rockport Publishers.
16. Griber, Y. A. (2023). Ekologicheskaya motivaciya cveta v gorodskoj koloristike [Ecological Motivation of Color in Urban Coloristics]. Project Baikal, 20(78), 60–65. Retrieved from https://doi.org/10.51461/issn.2309-3072/78.2235
17. de Marinis, M., Rinalduzzi, S., & Accornero, N. (2007). Impairment in color perception in migraine with and without aura. Headache: The Journal of Head and Face Pain, 47(6), 895–904. Retrieved from https://doi.org/10.1111/j.1526-4610.2007.00774.x
18. Shepherd, A. J. (2005). Colour vision in migraine: selective deficits for S-cone discriminations. Cephalalgia, 25(6), 412–423. Retrieved from https://doi.org/10.1111/j.1468-2982.2004.00831.x
19. Wilkins, A. J., Evans, B. J., & Plant, G. T. (2022). Potential uses for precision tinted lenses in a neurology clinic. touchREVIEWS in Neurology, 18(2), 93–102. Retrieved from https://doi.org/10.17925/USN.2022.18.2.93
20. Tappakhov, A. A., Popova, T. E., Steblevskaya, A. E., Nikolaeva, T. Y., Govorova, T. G. (2019). Primary headaches in clinical practice: modern views and new opportunities. Vestnik of North-Eastern Federal University. Medical Sciences, 3, 23–34. Retrieved from https://doi.org/10.25587/SVFU.2019.3(16).39464
21. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. (2018). Cephalalgia : an international journal of headache, 38(1), 1–211. Retrieved from https://doi.org/10.1177/0333102417738202
22. Verriest, G., Van Laethem, J., & Uvijls, A. (1982). A new assessment of the normal ranges of the Farnsworth-Munsell 100-Hue test scores. American Journal of Ophthalmology, 93(5), 635–642. Retrieved from https://doi.org/10.1016/s0002-9394(14)77380-5
23. Roy, M. S., Podgor, M. J., Collier, B., & Gunkel, R. D. (1991). Color vision and age in a normal North American population. Graefe's Archive for Clinical and Experimental Ophthalmology, 229, 139–144. Retrieved from https://doi.org/10.1007/BF0017054
24. Kinnear, P. R., & Sahraie, A. (2002). New Farnsworth-Munsell 100 hue test norms of normal observers for each year of age 5–22 and for age decades 30–70. British Journal of Ophthalmology, 86(12), 1408–1411. Retrieved from https://doi.org/10.1136/bjo.86.12.1408
25. Farnsworth, D. (1943). The Farnsworth-Munsell 100-hue and dichotomous tests for color vision. Journal of the Optical Society of America, 33(10), 568–578.
26. Farnsworth, D. (1957). The Farnsworth-Munsell 100-Hue Test for the Examination of Color Discrimination: Manual. Boston: Munsell Color Company.
27. Griber, Y. A., & Paramei, G. V. (2024). Colour discrimination in post-COVID-19 observers assessed by the Farnsworth-Munsell 100-Hue test. Russian Psychological Journal, 21(1).
28. McKendrick, A. M., Cioffi, G. A., & Johonson, C. A. (2002). Short-wavelength sensitivity deficits in patients with migraine. Archives of Ophthalmology, 120(2), 154–161. Retrieved from https://doi.org/10.1001/archopht.120.2.154
29. DaSilva, A. F., Nascimento, T. D., Jassar, H., Heffernan, J., Toback, R. L., Lucas, S., DosSantos, M. F., Bellile, E. L., Boonstra, P. S., Taylor, J. M. G., Casey, K. L., Koeppe, R. A., Smith, Y. R., & Zubieta, J. K. (2017). Dopamine D2/D3 imbalance during migraine attack and allodynia in vivo. Neurology, 88(17), 1634–1641. Retrieved from https://doi.org/10.1212/WNL.0000000000003861
30. Brandt, A. U., Zimmermann, H. G., Oberwahrenbrock, T., Isensee, J., Müller, T., & Paul, F. (2018). Self-perception and determinants of color vision in Parkinson's disease. Journal of Neural Transmission, 125(2), 145–152. Retrieved from https://doi.org/10.1007/s00702-017-1812-x
31. Tran, K. K. N., Lee, P. Y., Finkelstein, D. I., McKendrick, A. M., Nguyen, B. N., Bui, B. V., & Nguyen, C. T. O. (2024). Altered outer retinal structure, electrophysiology and visual perception in Parkinson's disease. Journal of Parkinson's Disease, 14(1), 167–180. Retrieved from https://doi.org/10.3233/JPD-230293
First Peer Review
Peer reviewers' evaluations remain confidential and are not disclosed to the public. Only external reviews, authorized for publication by the article's author(s), are made public. Typically, these final reviews are conducted after the manuscript's revision. Adhering to our double-blind review policy, the reviewer's identity is kept confidential.
The list of publisher reviewers can be found here.
The paper "Color vision in people with headaches" is submitted for review. The study provides a brief overview of the research and an analysis of the results of an empirical study. The subject of the study. The work is aimed at obtaining new data on possible changes in color vision in people with primary headaches. The author conducted an empirical study, and also expressed an experimental hypothesis. The work carried out made it possible to verify the assumption that people experiencing recurrent primary headaches of different nature have a changing perception of chromatic environmental parameters and color sensitivity. The differences may correlate with the experience of headaches, the frequency of their occurrence, the nature and quality of the pain experienced, their intensity and localization. The study allowed us to confirm the hypothesis put forward. The methodology of the study. The author analyzes a number of works that address the problem raised by the author: studying the relationship of various aspects of headache with individual components of the visual system, considering the parameters of visual discomfort ("visual stress", "sensitivity"), studying the specifics of perception of chromatic environmental parameters and color sensitivity, etc. The relevance of research. The problem raised in the article is relevant. Over the past few decades, clinical specialists and scientific researchers have been studying with particular interest the relationship of various aspects of headache with individual components of the visual system. Despite the availability of empirical studies, their number is insufficient. A review of the works published so far proves that the analysis of color sensitivity in people with headaches, in the vast majority of cases, is limited to patients with migraines. Comprehensive studies of color perception in people with other types of headaches have not been conducted. Only a few isolated cases of specific color sensitivity in people with cluster headaches have been described. Therefore, the conducted research is relevant. The scientific novelty of the study lies in the fact that the author shows a noticeable specificity in the perception of blue-green and blue shades in patients with severe, chronic and non-localized headaches: - the most significant changes in color perception were noted for blue shades in subjects with chronic pain; - differences in color perception between the group with headaches and the control group, mainly, touch the blue-yellow axis. The author notes that the detected violations may be related to the work of the dopaminergic system. Style, structure, content. The style of presentation corresponds to publications of this level. The language of the work is scientific. The structure of the work is clearly traced, the author highlights the main semantic parts. The logic of the work can be traced. The volume of the article meets the requirements for works of this level. The article begins with an introduction, which defines the relevance and problem of the study. The author notes that a significant part of the Russian population suffers from recurrent pain. This disease of the nervous system affects people of all races, income levels and geographical regions. The introductory section also includes a theoretical section, which presents an analysis of sources. The work carried out made it possible to characterize the following phenomena: the presence of similar visual triggers, the significant influence of certain visual qualities of the environment (characteristics of natural and artificial lighting, flickering light, certain visual images, the specific structure of the interior space of premises and workplaces), etc. The theoretical analysis allowed the author to note the connection between visual discomfort and color sensitivity, that is, the ability to perceive different color shades with different spectral composition of radiation. At the same time, the theory of effective coding receives empirical support, the essence of which is that visual stress is caused by shades that differ significantly from the usual ones – those that are usually found in the natural environment surrounding a person. It has also been established that tinted lenses affect the feeling of visual discomfort and the frequency of headaches. The author described the problem, as well as the purpose and hypothesis. The second section is devoted to the description of materials and methods, as well as the results of empirical research. The study involved 65 people aged 17 to 66 years, who have recently experienced headaches of different intensity, nature and quality with different frequency and with different experience. The respondents filled out a detailed questionnaire that included an expanded set of questions about various aspects of headaches. Data collection was carried out using the standard clinical Farnsworth-Mansell color vision test for 100 shades. The results were analyzed using specialized computer programs: the total error was calculated, partial errors along the blue-yellow and red-green axes were calculated, and partial errors for individual tones were also calculated. The data revealed: - the mean value and standard deviation of the square root of the total number of errors for healthy normal trichromates; - correlation between the frequency of headache occurrence (episodic, frequent, chronic) and the value of the total error score; - correlation between the intensity of headache (mild, moderate, severe) and the value of the total error score; - the value of the total error score correlated with the localization of headaches; - the absence of a statistically significant correlation between the experience of headaches and the magnitude of the total error score; - an insignificant correlation of the total error score with age, gender, nature and quality of headaches (aching, pressing, throbbing, acute, bursting), normal behavior during an attack (drowsiness, emotional arousal, anxiety, fear) and heredity headaches. The author identified: - partial errors along the blue-yellow and red-green axes in patients with different frequency of headaches; - partial errors along the blue-yellow (B-Y) and red-green (R-G) axes in patients with varying headache intensity; - the average value of the partial error for individual tones in patients with different frequency of headaches; - the average value of the partial error for individual tones in patients with different frequency and intensity of headaches; - the average value of the partial error for individual tones in patients with varying degrees of headache localization. In conclusion, the author concluded that the new data obtained on changes in color vision may be useful for understanding not only the pathophysiology of headache. These results can be used in the development of alternative treatment methods. For example, to choose the optimal color of tinted lenses, which are offered to patients to relieve headaches and reduce the frequency of seizures. Bibliography. The bibliography of the article includes 31 domestic and foreign sources, a small part of which have been published in the last three years. The list contains mainly articles and abstracts. In addition, there are also monographs and online sources. The sources are mostly incorrectly and heterogeneously designed. Appeal to opponents. Recommendations: 1) develop recommendations based on the results of the study; 2) there are syntactic, stylistic and semantic inaccuracies in the work (for example, "... makes up only 14% of all cases"); 3) arrange the list of references in accordance with the requirements. Conclusions. The problems of the article are of undoubted relevance, theoretical and practical value; it will be of interest to specialists who deal with the problems of headache correction. The article may be recommended for publication. Taking into account the highlighted recommendations and making appropriate changes, it is possible to submit to the editorial board a research article characterized by scientific novelty and significance.
Second Peer Review
Peer reviewers' evaluations remain confidential and are not disclosed to the public. Only external reviews, authorized for publication by the article's author(s), are made public. Typically, these final reviews are conducted after the manuscript's revision. Adhering to our double-blind review policy, the reviewer's identity is kept confidential.
The list of publisher reviewers can be found here.
The reviewed article is devoted to an urgent problem – the identification of triggers that provoke diseases of the nervous system. The authors pay attention to the study of environmental factors, their connection with various aspects of headache. The authors emphasize the difference between sensitivity to external stress in people suffering from headaches and people from the corresponding control age group, analyze the influence of different colors as triggers of headache, consider provoking household factors. The novelty of the work lies in the study of factors not only for patients with migraine, but also for patients with primary headaches. The structure of the article meets the requirements for publication. The authors describe in detail the experimental part, provide calculations and analysis of quantitative estimates of the results. The sample used is sufficient, the description of the experimental part of the FM-100 test allows you to reproduce the results of the study. The advantage of the work is the analysis of the correlation of quantitative estimates with the intensity and localization of pain, while at the same time showing the absence of dependence of the total error score on the length of pain. The result of the dependence of partial errors for different color sets on the frequency of pain is interesting, as well as a graph of the dependence of errors for different shades for patients with different frequency of pain. The greatest sensitivity to short-wavelength waves is noted, and recommendations are given for possible reduction of the effects of pain attacks. The style of presentation meets the requirements. There are illustrations, the quality is sufficient. The bibliography contains 31 sources, mainly foreign publications in peer-reviewed journals. There are links in the text. Remarks. Materials and methods. In each of the samples under consideration, the number of women significantly exceeds the number of men. It is necessary to clarify whether such a ratio has a significant impact on the result. The evaluation procedure is described in detail, but perhaps an illustration (photo or diagram) should be added that clearly shows the means for conducting the FM-100 test. The formula for calculating the total TES error is not visible. It is not clear how the ranges for individual tones were selected (preset values, according to the number of chips, another criterion), because for some ranges the chips are located in different pencil cases, and from the description of the testing tools it is known that the first and last in each pencil case are fixed, therefore, the error of their location is excluded. Then for the range, for example, 36-45 out of 10 chips for two (42 and 43), the position is fixed. And in the range 18-26, 2 chips out of 9 were recorded. How was the calculated total error compared with the known data (Table 1 shows the norm values for three studies, but for some groups the ranges of values differ)? It should be noted in the text. The description does not indicate the criterion for dividing patients into groups (episodic, frequent, chronic pain), although the frequency of pain for these groups is mentioned when calculating partial errors. It is advisable to indicate this above Fig.1. Fig. 4 to compare the analyzed axes relative to the rest, it is recommended to add the results. The remark is of a recommendatory nature. Fig. 6 – what explains the decrease in errors for the B-PB, PB-P ranges in patients with episodic and frequent pain relative to the control group? In the bibliography, it is necessary to check the correctness of the spelling of the output data. The article will be of interest to a wide range of readers. The article corresponds to the profile of the Journal and can be published after making edits, re-reviewing is not required.
|








