|
Psychology and Psychotechnics
Reference:
Kim K.V., Petrova A.A.
Cognitive impairment in elderly patients suffering from Alzheimer's disease
// Psychology and Psychotechnics.
2022. ą 2.
P. 79-88.
DOI: 10.7256/2454-0722.2022.2.36877 URL: https://en.nbpublish.com/library_read_article.php?id=36877
Cognitive impairment in elderly patients suffering from Alzheimer's disease
Kim Kseniya Vasil'evna
ORCID: 0000-0002-4511-4138
PhD in Psychology
Associate Professor, Department of Psychology and Social Sciences, Northeastern Federal University named after M.K.Ammosov
677010, Russia, g. Yakutsk, ul. Kulakovskogo, 42, of. 405

|
kv.kim@s-vfu.ru
|
|
 |
|
Petrova Alina Alekseevna
student, Department, Northeastern Federal University named after M.K.Ammosva
677013, Russia, respublika Sakha (yakutiya), g. Yakutsk, ul. Kulakovskogo, 42, of. 405
|
|
Linapetrova1997@gmail.com
|
|
|
|
DOI: 10.7256/2454-0722.2022.2.36877
Received:
16-11-2021
Published:
18-06-2022
Abstract:
The purpose of the study: to study destructive forms of cognitive impairment in old age. Materials and methods. A study of 38 people was conducted, of which 16 were men and 22 were women. The control sample consists of 23 people, of which 8 are men and 15 are women. The definition of the control sample was based on the fact that this category of people had cognitive impairments that are the result of other age-related changes that are not the result of AD, whereas the experimental sample needed to have cognitive impairments that are the result of AD. The experimental sample consisted of 15 people, 7 men, 8 women. In the process of MMSE testing, 6 subjects (15.8%) entered the first group, 10 subjects (26.3%) entered the second group, and 22 (57.9%) entered the last group. 42.1% of respondents had mild Alzheimer's type dementia, while 57.9% of respondents had cognitive impairment due to age-related changes. According to the indicators obtained by the method of the short scale of assessment of mental status (Mini-Mental State Examination, MMSE), it can be concluded that memory, attention and orientation in time and space are primarily reduced. Data on the Frontal Dysfunction Battery (FAB) technique showed the absence of a grasping reflex in 29 out of 38 subjects (76.3%), so the presence of a grasping reflex most often indicates a severe degree of Alzheimer's type dementia.
Keywords:
Cognitive impairment, neurodegenerative diseases, old age, Alzheimer's disease, clinical picture, dementia, pre - dementia, destructive forms, cognitive impairment, praxis
This article is automatically translated.
Introduction According to Rosstat data in Russia, as of 2020 there are over 27 million people over the age of 60 [6]. Improving medical care, as well as reducing the risk of serious somatic diseases, led to the appearance of significant disorders associated with cognitive functions. According to statistics, the incidence of dementia doubles with an increase in age by 5.9 years – from 3.1 per 1,000 person-years aged 60-64 years to 175.0 per 1,000 person-years aged 95 years or more [1]. Of greatest interest is the study of neurodegenerative diseases, a group of mostly slowly progressive, hereditary or acquired diseases of the nervous system. Neurodegenerative diseases are the most common cause of cognitive impairment in old age. Common to these diseases is the progressive death of nerve cells (neurodegeneration), leading to various neurological symptoms — primarily dementia and impaired movement [5]. The clinical picture of cognitive impairment varies depending on the type of degenerative brain diseases. Thus, dementia with Lewy bodies (DTL), which is the second most common, is diverse and characterized by a combination of cognitive, motor, behavioral and autonomic disorders. In the later stages of the disease, dementia is characteristic, with violations of visual attention, spatial gnosis and praxis, which are episodic in nature, coming to the fore [2]. In frontotemporal dementia (LVD), behavioral disorders, a decrease come to the fore, violations of voluntary attention, visual-spatial disorders are noted in cognitive functions. [1]. Alzheimer's disease (hereinafter AD) ranks first in the list of causes of dementia and is responsible for approximately 40% of all cases of dementia [9]. The development of AD is characterized by the passage of three stages (E. Sternberg): early (initial), intermediate (moderate dementia), late (severe dementia). Kotov A. S. identifies four stages in AD: pre-dementia, early dementia, moderate dementia, severe dementia [4]. The dynamics of the course of the disease is quite natural. As a rule, the trend of BA development is gradual and you flow from a lighter stage to a more severe one The most common initial symptoms include: forgetfulness, difficulties in concentration and a limited amount of attention, difficulties in learning and assimilation of new material, difficulties in maintaining conversation, communication, solving problems in the workplace, inability to perform complex cognitive tasks, follow instructions; disorientation in the chronology of events and space; slight violations of coordination and praxis; passivity, withdrawal, mood swings, depression or delusional disorders [2, 3, 4, 5, 7]. The early stage of the disease is quite difficult to diagnose [7]. As a rule, the first symptoms are often confused with the manifestation of aging or a reaction to stress, despite the manifestations long before the diagnosis (for 8 years). Accurate diagnosis is possible when conducting extensive neuropsychological testing. [8, 10, 11]. The stage of moderate (prodromal) dementia is characterized by an aggravation of the condition. Paraphasias are also connected to aphasia (replacing forgotten words with incorrect ones). Mnestic problems are getting worse, which is manifested by not recognizing relatives and loved ones. Previously unaffected long-term memory is also impaired. In addition, the coordination of movements becomes obvious, which leads to a constant need for help in performing everyday tasks. These disorders reach such a degree of severity that patients need constant assistance in daily activities, maintaining personal hygiene, dressing. The somatic state worsens: appetite, sleep and wakefulness are disturbed [4, 5, 7]. At the stage of severe dementia, a person loses the ability to serve himself independently. Speech disorders fade to the extent of using only individual phrases or even individual words, in the future speech disappears completely. However, the emotional response remains, the person is able to respond to the addressed speech and respond nonverbally. There is incontinence of stool and urination. In the final stage, a person becomes bedridden, and care is reduced only to maintaining vital activity and ensuring a decent quality of life (palliative care) [2, 3, 5]. The question of the etiology of BA is one of the discussed. To date, the causality of the disease appears to doctors as follows: as a result of deposition or modification of protein, cellular metabolism is weakened, which contributes to a decrease in cell productivity, which, of course, affects its work. First of all, the ability to form intersynaptic connections, the main ones in the memory mechanism, is impaired. A critical decrease in the number of nerve cells, as well as a violation of the interaction between them, leads to a disruption of the brain, which affects the cognitive abilities of the patient [4]. Study The aim of the study is to study the features of cognitive processes in the elderly with AD Subject: features of cognitive impairment in degenerative diseases Object: elderly people (60-75 years old) Materials and methods The sample size was 38 people, of which 16 were men and 22 were women. The control sample consists of 23 people, of which 8 are men and 15 are women. The definition of the control sample was based on the fact that this category of people had cognitive impairments resulting from age–related changes, whereas the experimental sample needed to have cognitive impairments resulting from AD. The experimental sample consisted of 15 people, 7 men, 8 women.
As empirical research methods, a short scale of assessment of mental status (Mini-Mental State Examination, MMSE) was used to assess the level of cognitive impairment of the frontal Dysfunction Battery (FAB), to determine the severity of cognitive impairment associated with impaired function of the anterior brain and frontal-subcortical connections. For a more reliable diagnosis of cognitive impairment, it is of great importance to compare the indicators obtained by two methods. And also, as mathematical methods of processing, criteria such as correlation analysis by Spearman's criterion to identify relationships and the Mann –Whitney U–test to identify differences in cognitive impairment in the control and experimental samples were chosen. 42.1% of respondents had mild Alzheimer's type dementia, while 57.9% of respondents had cognitive impairment due to age-related changes. As we said above, dementia and cognitive impairment are synonymous concepts in some way, but the dynamics of cognitive decline in AD is fundamentally different from the same dynamics of decline in age-related changes. If there is a certain sequence of cognitive function loss in AD, then with age-related changes we cannot trace a generally accepted pattern. Mild Alzheimer's type dementia (the stage of early dementia) is characterized primarily by the loss of short-term memory, and many have speech disorders (decreased fluency, vocabulary). In addition, there is a certain awkwardness in the movements due to problems with the planning of the motor act. 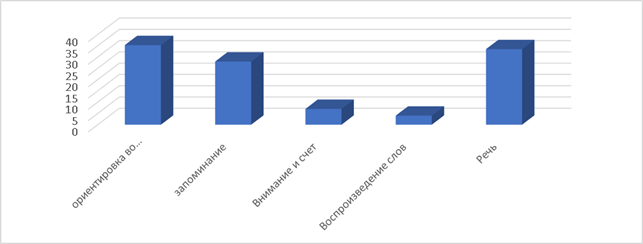
Fig.1. Analysis of comparison of the data obtained by the method "Short scale of assessment of mental status (Mini-Mental State Examination, MMSE)" (n=15) According to the indicators obtained by the method of the short scale of assessment of mental status (Mini-Mental State Examination, MMSE), it can be concluded that memory and attention are primarily reduced in the choice. 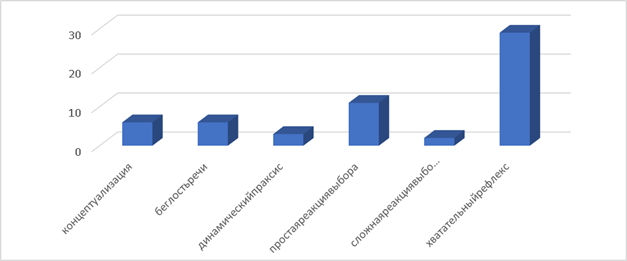
Fig.2. Analysis of comparison of the data obtained by the method "Frontal Dysfunction Battery (Frontal Assitssment Battery, FAB)" (n=15) The data on the method of frontal dysfunction Battery (Frontal Assitssment Battery, FAB) is most correctly considered by the highest indicator. The highest number of correct answers was obtained by the absence of a grasping reflex 76.3% of the subjects, since the presence of a grasping reflex most often indicates a severe degree of Alzheimer's type dementia. However, the simple and complex choice reaction carried out suggests that motor (coordination) problems are present. 28.9% of the subjects answered correctly to a simple choice reaction, while only 5.3% answered correctly to a complex choice reaction. A significant decrease in the results, with the complication of the choice reaction, indicates the progressive nature of the violations. The results obtained In the study of the severity of cognitive impairment depending on age, no correlations were found (0.088, at p) of low statistical significance (0.01). Thus, we found out that in our sample there was no dependence of the severity of cognitive impairment on age, but this indicator is statistically low. In the course of the study, the differences between the two samples (control and experimental samples) were revealed. The data obtained by the Mann–Whitney U–test indicate that there are significant differences in the level of cognitive impairment between the two samples. The average rank of short–term memory in the control sample is 27.36, whereas in the experimental sample it is 8.69, at p=0.001. Thus, there is a decrease in the tested variable in the experimental sample. There are differences in the level of fluency of speech in the two samples. The average rank indicator in the control sample is 27.44, and in the experimental sample – 13.73, at p = 0.001, which indicates significant differences in the level of fluency of speech. The indicators of the level of conceptualization (control sample - 26.94, experimental sample – 14.09) indicate that there is a difference in the two samples with a high degree of asymptotic significance of 0.001. The most obvious are the differences in the level of short-term memory. In the experimental sample, the indicator is lower by more than two times. Conceptualization comes second in terms of the level of difference, followed by fluency of speech. Differences were found in all the variables being tested. The study revealed the existence of a relationship between conceptualization (generalization) and the severity of cognitive impairment, there is a moderate two-way positive relationship (0.629**, at p=0.000). Thus, the level of generalization is determined by the degree of severity of cognitive impairment. A two-way positive relationship was also found between fluency of speech and the degree of severity of cognitive impairment, however, it is no longer moderate, but strong (0.735**, at p= 0.000), fluency of speech depends on the degree of severity of cognitive impairment and vice versa. Generalizing, we can say that there is a certain relationship between cognitive impairment and fluency of speech, conceptualization, and the level of short-term memory. The differences between the two samples between the variables being tested turned out to be significant. It should be noted that there was no correlation between age and the level of cognitive impairment. Conclusions: A significant difference was revealed in terms of: conceptualization, fluency of speech and short-term memory
The study established the relationship of conceptualization, fluency of speech and short-term memory with the severity of cognitive impairment, the level of praxis and the degree of severity of cognitive impairment and the severity of cognitive impairment. Conclusion To date, BA is in the first place among degenerative diseases in the elderly. Within the framework of this study, data were obtained on the characteristics of cognitive impairment in the elderly in people with and without a diagnosis of AD. The analysis made it possible to identify differences in the severity of the characteristics of cognitive impairment, as well as the relationship between different indicators.
References
1. Bogolepova, A.N. Modifitsiruemye faktory riska i sovremennye podkhody k terapii dementsii // Meditsinskii sovet. – 2015. – ą 10. – S. 28-33
2. Zakharov, V.V. Kognitivnye narusheniya pri neirodegenerativnykh zabolevaniyakh // Meditsinskii sovet. – 2013. – . – ą 4. – S. 30-35
3. Koberskaya, N. N. Bolezn' Al'tsgeimera: novye kriterii diagnostiki i terapevticheskie aspekty v zavisimosti ot stadii bolezni // Meditsinskii sovet. — 2017. — ą 10. — S. 18-24.
4. Kotov, A. S. Bolezn' Al'tsgeimera: ot teorii k praktike // Meditsinskii sovet. — 2015. — ą 18. — S. 41-44.
5. Tyuvina, N. A, Balabanova, V. V. Dementsii al'tsgeimerovskogo tipa: sovremennoe sostoyanie problemy // Nevrologiya, neiropsikhiatriya, psikhosomatika. — 2014. — ą 1. — S. 61-67.
6. Chislennost' pozhilogo naseleniya. // Federal'naya sluzhba gosudarstvennoi statistiki: [sait]. — URL: https://rosstat.gov.ru/folder/12781
7. Shternberg, E. Ya. Klinika dementsii presenil'nogo vozrasta. Moskva : Meditsina, 1967. — 247 c.
8. Yakhno, N. N. Kognitivnye rasstroistva v nevrologicheskoi klinike // Nevrologicheskii zhurnal. — 2006. — ą 11. — S. 4-12.
9. Yakhno,N 30, I. S. Preobrazhenskaya, V. V. Zakharov [i dr.]. Rasprostranennost' kognitivnykh narushenii pri nevrologicheskikh zabolevaniyakh (analiz raboty spetsializirovannogo ambulatornogo priema) // Nevrologiya, neiropsikhiatriya, psikhosomatika. — 2012. — ą 2. — S. 30-34.
10. Gatz M, Reynolds CA, Fratiglioni L, et al. Role of genes and environments for explaining Alzheimer disease. Arch Gen Psy chiatry. 2006 Feb. 63(2): 168-74.
11. Wilson RS, Barral S, Lee JH et al. Heritability of different forms of memory in the Late Onset Alzheimer’s Disease Famil y Study. J Alzheimers Dis. 2011.; 23(2): 249-55.
|








